eISSN: 2093-8462 http://jesk.or.kr
Open Access, Peer-reviewed
eISSN: 2093-8462 http://jesk.or.kr
Open Access, Peer-reviewed
Yong-Ku Kong
, Sung Yong Lee
, Dae-Min Kim
, Kyeong-Hee Choi
10.5143/JESK.2017.36.1.53 Epub 2017 March 02
Abstract
Objective: The purpose of this study is to build basic data to systematically develop a hand function evaluation tool by determining the effects of age, gender and target force level on the difference in hand function according to the target force level.
Background: Precise and objective evaluation of hand functionality is a very important factor in quantifying treatment progress in patients or elderly people, and in verifying treatment effects. However, most hand function evaluations lack objectivity and accuracy, and therefore it is difficult to properly treat patients according to the given situation.
Method: Sixteen healthy subjects (eight elderly and eight young people) participated in this study to evaluate the effects of age, gender, and target force level on tracking performance through rRMSE in terms of the tracking force and actual exerted force, by carrying out a task of maintaining six different target force levels for 20 seconds.
Results: The result of this experiment indicated that elderly people and women had a lower ability to maintain a certain level of force than young people and men by 16% and 10%, respectively. The target force level results showed that the tracking error of the lowest force level (5% MVC) was significantly higher than that of 15% MVC, which in turn showed a higher tracking error than that of the higher target force levels.
Conclusion: The results of this study can thus be utilized to develop a rehabilitation program for elderly people or other patients.
Application: The authors expect that the results of the present study will be valuable to develop a rehabilitation program and hand function evaluation tool.
Keywords
Aging Gender Tracking error Controlled force exertion Rehabilitation
Humans receive sensory information concerning their motions in daily life through receptors such as the skin or eyes, and the information that is captured is integrated in the brain. A signal is then sent to induce the proper muscular response. However, the message sent from the brain to the muscle is distorted by internal noise, and such noise increases motor output variability, and causes a reduction in the ability to precisely control the intended movement (Christou, 2011; Kennedy and Christou, 2011). As a consequence, motor output variability is an important factor in deciding the performance in a task that requires accuracy. If the variability is large, the activities of daily living (ADLs) can become restricted due to uneven force or movement. Christou (2010) defined motor output variability as the unintended change that takes place in a voluntary contraction; whereas, Van Beers et al. (2004) defined it as noise overlapping on the exercise order. Therefore in order to enhance the amplitude and direction of the force and the accuracy of time to exert such force, motor output variability should be minimized (Schmidt et al., 1979; Carlton and Newell, 1993).
In particular, motor output variability is known to increase according to aging (Galganski et al., 1993; Hortobágyi and DeVita, 1999; Christou and Carlton, 2001; Vaillancourt and Newell, 2003). An elderly person tends to exert excessive hand grip strength or show slow movement, and when carrying out a task maintaining force, such phenomena reduce accuracy, and cause high variability in performance (Jagacinski et al., 1995; Smith et al., 1999; Ranganathan et al., 2001; Krampe, 2002; Kurillo et al., 2004a; Shim et al., 2004; Voelcker-Rehage and Alberts, 2005).
The motor control function could be measured with using controlled force exertion (CFE) test. The CFE test is used to evaluate the upper limb's coordination (Kubota et al., 2013). The CFE test demands that the participants match their submaximal grip strength values to the demand values on a computer display (Nagasawa et al., 2000).
Sosnoff and Newell (2006) conducted a task that maintained the target level (5% and 25% MVCs) by adjusting the abduction force of the index finger. Their results revealed that the elderly people group (70.9yr, force CV: 0.06) exhibited a significantly higher variability than the young people group (24.9yr, force CV: 0.04). The elderly people also had high variability in the low target force level (5% MVC). Galganski et al. (1993) performed a study using the abduction force of the index finger by asking participants to carry out a task while maintaining constant force for 20 seconds at four force levels (4%, 20%, 35%, and 50% MVCs). The results of the study indicated that the force controlling ability of the aged (67yr) to constantly maintain the force was lower than that of young people (28yr). The difference in force control ability between elderly people and young people at the lower force levels was remarkable.
In addition to aging, damage to central nerves, hand injuries, or neuromuscular disease are also the causes of decline in hand function. Kurillo et al. (2004b) conducted a ramp task and a sine task to compare the grip force control abilities of neuromuscular patients and healthy people. The results showed more tracking errors from neuromuscular patients, and some of these patients showed more than two times higher errors. Nagasawa and Demura (2005) carried out a controlled force exertion test for grip force control that targeted patients with encephalomeningitis, schistorrachis and cerebral palsy, and healthy people. According to the results of the research, the performance (sum of target values and exerted value) of the patients with encephalomeningitis and schistorrachis was significantly higher than that of the healthy people.
Precise and objective evaluation of hand functionality is a very important factor in quantifying treatment progress in patients or elderly people, and in verifying treatment effects. However, most hand function evaluations lack objectivity and accuracy (McPhee, 1987), and therefore it is difficult to properly treat patients according to the given situation (Kurillo et al., 2005). In the clinical field, the most commonly used method to evaluate hand function is to measure the maximum grip force. The maximum grip force offers information of muscular contractions for a short time of only six seconds, while more sophisticated grip force control is needed in everyday life. This is a limitation of the measuring of maximum grip force.
In addition, many researchers have mainly conducted studies using the abduction force or pinch force of the index finger only, so there is a limitation in the synergetic effect, such as in the enslaving effect not being fully reflected when multi-finger force is exerted. People in everyday life mostly use all fingers, rather than just the index finger. For this reason, an evaluation of multi-finger force should be considered to reflect hand force controlling ability or functionality.
The purpose of this study is to build basic data to systematically develop a hand function evaluation tool by determining the effects of age, gender and target force level on the difference in hand function according to the target force level.
2.1 Participants
A total of 16 healthy adults without musculoskeletal disorders in the upper arms participated in this study. The young group and elderly group were recruited through advertising from the university and a senior welfare center, respectively. The young group consisted of 8 healthy adults (4 males and 4 females) with a mean age of 22.3 years (SD=1.4), while the elderly group was composed of 8 participants (4 males and 4 females) with a mean age of 67.9 years (SD=2.9), respectively. Each of the participants was paid for their participation at the rate of $30.00 per hour. Informed consent was obtained at the beginning of the experiment, and anthropometric measurements, including height, weight, hand length, hand width, and hand thickness were measured. Table 1 provides further details.
|
|
Age |
Height (cm) |
Weight (kg) |
Hand length (mm) |
Hand width (mm) |
Hand thickness |
||||
|
Right |
Left |
Right |
Left |
Right |
Left |
|||||
|
Young |
Female |
22.3±1.9 |
164.6±4.5 |
56.9±12.2 |
172.4±8.4 |
172.1±6.1 |
74.0±1.8 |
74.3±4.3 |
27.9±2.7 |
27.4±4.2 |
|
Male |
22.3±1.0 |
178.6±2.3 |
78.0±19.9 |
185.0±2.0 |
182.7±0.7 |
82.5±5.7 |
82.1±5.0 |
33.3±4.0 |
31.0±2.3 |
|
|
Elderly |
Female |
68.3±2.5 |
163.1±6.0 |
71.1±10.0 |
182.0±4.3 |
180.4±5.0 |
81.6±1.7 |
82.0±2.8 |
28.9±3.7 |
29.2±2.7 |
|
Male |
67.5±3.7 |
165.4±8.6 |
70.0±8.3 |
177.4±8.3 |
177.3±6.5 |
84.7±1.9 |
86.4±4.2 |
32.8±1.2 |
31.6±1.1 |
|
2.2 Apparatus
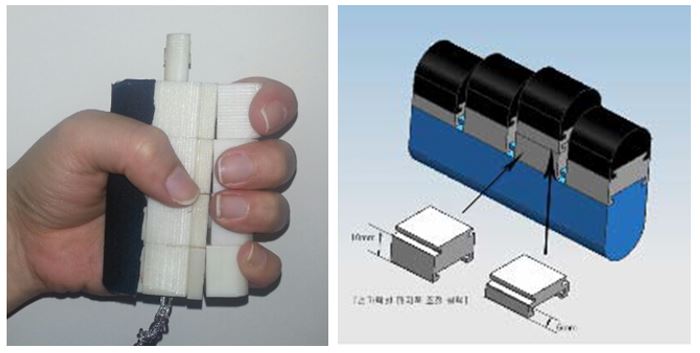
In this study, a Multi-Finger Force Measurement (MFFM) System developed by Kim and Kong (2008) was applied to measure grip strength, and to evaluate controlled force exertion for various target force levels. The MFFM system is composed of four sub-miniature load cells (Model 13, Honeywell International, ranging from 0~22.7kg, with a 9.5mm diameter 2.75mm thick cylindrical shape) to measure individual finger forces with a sampling rate of 10Hz (Figure 1). Each load cell was calibrated by known weights (1~5kg) on a custom-made calibration fixture, and each load cell exhibited a high level of linearity between the output data and the known weight that was applied (R2 > 0.99). The output signals were collected using an NI USB-6008 DAQ board, and were displayed on screen using custom-made software written in LabVIEW 8.5 (National Instruments, Austin, TX, USA).
2.3 Experimental Procedure
All participants were provided with a brief description of the experimental purpose and procedures, and practice tests were then performed for familiarization with the experiment. To measure the maximum grasping force, participants were asked to perform their maximum voluntary contraction (MVC) for 5 seconds with three repetitions for both hands. To reduce the effect of muscle fatigue, the participants were also provided 3 minutes of rest time between repetitions (Trossman and Li, 1989). This study used the mean value of three exertions as the MVC value. Target forces were determined for each participant based on the MVC value obtained with the maximum grasping task for each participant, of 5%, 15%, 25%, 35%, 45%, and 55% MVCs.
For the CFE test, participants were sitting in a chair in front of a computer screen. The elbow was positioned in a 90° flexion, and the wrist and forearm were in a neutral position. The participants were asked to exert a grip force while attempting to minimize the difference between the target force (FT) and their exerting force (FE). The task screen displayed the target forces in white, and the exerted force responses in red color (Figure 2). The duration of each trial was of 20 seconds, and the data from the middle 10 seconds was collected and used to measure the tracking error in this study, excluding the first and the last 5 seconds of each trial. Six different target forces (5%, 15%, 25%, 35%, 45%, and 55% MVCs) were randomly selected according to the maximum voluntary contraction that was measured in the maximum grasping task for each participant. The CFE test for both hands was performed for both hands with two repetitions for each target level in random sequences, with a 2-minute rest time between trials. Hence, each participant performed 24 exertions (2 hands × 6 target force levels × 2 trials) for this study. The participants were instructed to track the target force as accurately as possible for 20 seconds, and the acquisition data were automatically saved as an Excel file. LabVIEW software (National Instrument, Austin, Texas) was used to analyze the tracking error (rRMSE) between the target force (FT) and the exerted force (FE).

2.4 Data analysis
A repeated-measures analysis of variance (ANOVA) was used to evaluate the effects of age, gender, and target force level on the tracking error (rRMSE). Multiple comparisons were carried out using Tukey's test, and the significance level of all tests was set to p < 0.05.
Equation (1) defines the tracking error (rRMSE) that was the difference between the target force () and the exerted force (
) over the trial time T. The tracking error was normalized by the target force, in order to allow comparison between the results obtained for different target levels and participants. A lower tracking error indicates better activation control of the corresponding muscles and improved hand functionality (Jones, 2000; Kriz et al., 1995).
rRMSE (relative root mean square errors) = ····· Equation (1)
where, = exerted force,
= target force, and
= number of data.
The subject was considered as a random effect, while age (young and elderly), gender (male and female), and target force level (5%, 15%, 25%, 35%, 45%, and 55% MVCs) were considered as fixed effects.
3.1 Maximum grip strength
A statistical analysis of the maximum grip strength indicated that the main effect of gender was a statistically significant factor in this study (p < 0.001). The maximum grip strength for females (178.3N) was 69.3% that of males (257.2N). Although the main effects of age and handedness on the maximum grip strength were not statistically significant, the elderly group (209.6N) generally exhibited about 91.2% that of the young group (229.9N), and the dominant hand (222.7N) was about 5% stronger than the non-dominant hand (212.8N), respectively.
3.2 Tracking error
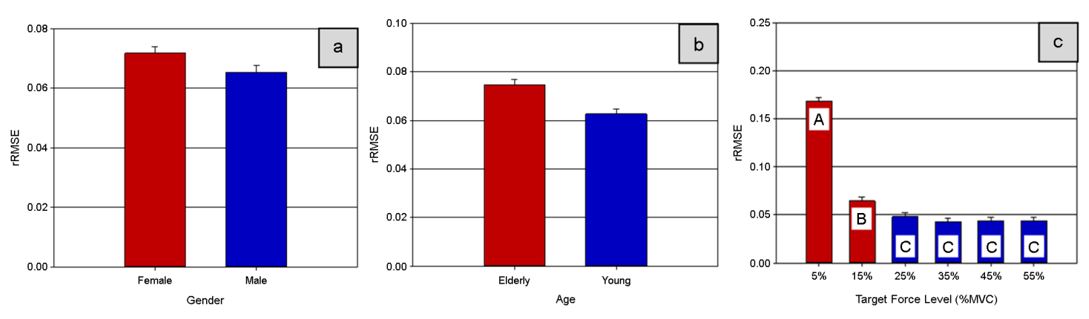
The statistical analysis showed that the main effects on the tracking error of gender (p = 0.046), age, target force level (all p-values < 0.001), and the interaction effects of age and target force level (p < 0.001), and of gender and target force level (p = 0.009) were statistically significant at a significance level of α= 0.05. The effect of handedness was not statistically significant (p = 0.07).
The tracking error for females (0.072) was 10% higher than that for males (0.065). Figure 3a shows that males were found to have a better ability to control finger muscles than females, while Figure 3b shows that in the analysis according to age, the elderly group (0.075) showed a 16% higher tracking error than that of the young group (0.063). For the target force levels, the tracking errors decreased as the target force levels increased from 5% to 55% MVCs. Tukey's multiple comparison test revealed that the largest tracking error (0.169) was obtained at 5% MVC, and the tracking error (0.065) at 15% MVC was also significantly larger than those (ranges from 0.042~0.048) at 25%~55% MVCs. Figure 3c shows that there was no significant difference between tracking errors for 25%, 35%, 45%, and 55% MVCs.
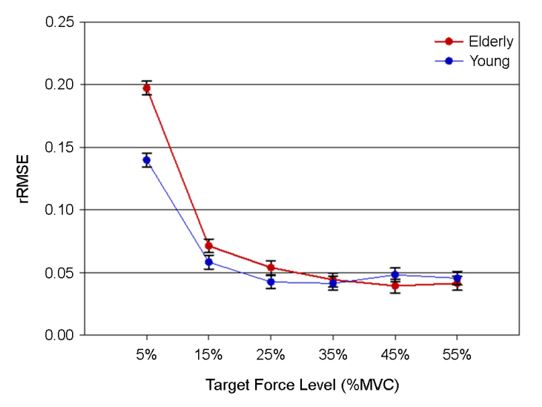
The interaction effect between the target force level and age was statistically significant (p < 0.001). Overall, the average tracking errors of the elderly group were significantly larger than those of the young group, except for the 35% and 55% MVC force levels. In particular, Figure 4 shows that the difference in tracking error between the elderly and young groups at the lowest target force level (5% MVC) was relatively greater than that between the elderly and young groups at other target force levels.
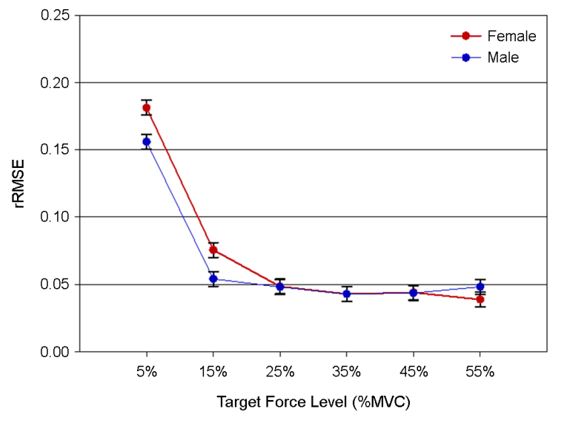
Interestingly, Figure 4 shows that the interaction effect between the target force level and gender (Figure 5), which was also statistically significant (p = 0.009), showed a similar pattern to the interaction effect of the target force level and age. The female group showed a significantly larger tracking error (28.5%) than the male group at the target force level of 15% MVCs, while the female group showed a smaller tracking error than the male group at the largest target force (55% MVC). Although there were no significant differences in tracking errors between male and female at the lowest target force level (5% MVC), females showed a larger tracking error (13.8%) than males.
Although the interaction effect between gender and age was not statistically significant (p = 0.06), the differences in tracking error between females in the elderly (0.081) and young (0.068) groups were generally more obvious than those (0.063 and 0.062 for elderly and young groups, respectively) for the male group.
4.1 Grip force
The grip force measurement is a representative method that can be used to objectively evaluate the force and function of a hand (Lee et al., 1995) to identify the degree of injuries or diseases, and to evaluate the effect of treatment.
Grip force is known to decrease due to aging; it continuously increases until the late teens, shows relatively stable measured levels from the 20s to 40s, and then a downward trend after the 50s (Mathiowetz et al., 1985; Lee et al., 1995). Martin et al. (1985) claimed that the decrease in grip force according to aging is due to the decrease in the amount of muscle from aging. Lexell et al. (1983) also found that a decrease in the size and number of muscular fibers is the cause of a decrease in grip force. Galganski et al. (1993) reported that elderly people (67yr, range: 60~75yr) showed an 18% smaller grip force than young people (28yr, range: 20~37yr). This study also found differences in the maximum grip force according to age, and elderly people (67yr, range: 65~71yr) revealed about 10% smaller maximum grip force than young people (22yr, range: 19~23.7yr).
Gender is also a main factor affecting the maximum grip force. Many studies reported that women exerted only 56~70% of men's grip force (Pheasant and Scriven, 1983; Härkönen et al., 1993; Talsania and Kozin, 1998; Kong and Lowe, 2005). The difference in grip force according to gender is caused by differences in the muscles' physiological cross-sectional area (Miller et al., 1993), the size of the hand (Desrosiers et al., 1995), and the height and weight of men and women (Balogun et al., 1991; Hanten et al., 1999). In particular, the difference by gender in muscle strength in the upper limbs compared with lower limbs was more obvious based on previous studies (Levine et al., 1984; Heyward et al., 1986). This study found a difference in grip force according to gender as well: Women exerted 69.3% of the maximum grip force compared to men, which is a similar result to the results of 66% and 68% reported by McMullin and Hallbeck (1992) and Hall (1997), respectively.
The grip force of the dominant hand was 222.7N, which is 5% larger than that of the non-dominant hand in this study. Crosby et al. (1994) asserted that the grip force of the dominant hand was 6% stronger than that of the non-dominant hand, which is similar to the results of this study.
4.2 Limitations of grip force as indicator of hand function
Although grip force is used as an indicator to evaluate the reduction in physical function or hand function according to aging or disease (Kallman et al., 1990), there are some limitations of using the grip force to estimate the reduction of hand functionality. First, ADLs more frequently use submaximal strength than maximum grip force. Since ADLs, like writing or eating with a spoon, require relatively less grip force control (Oldfield, 1971), judging the performance during daily living or hand function with only the maximum grip force is limited. The measurement for maximum grip force can be used to obtain muscle contraction information for 5~6 seconds over a short period of time, and therefore, it is insufficient to fully evaluate the hand function. Second, as the maximum grip force is measured, excessive force should be imposed upon the hand. In particular, elderly people's bone density and amount of muscle decrease mean that maximum grip force measurement may affect hand injuries as a risk factor.
4.3 Controlled Force Exertion (CFE) test
Studies on the Controlled Force Exertion (CFE) test have been carried out to actively find an alternative to complement the limitations in grip force measurement (Halaney and Carey, 1989; Nagasawa and Demura, 2002; Kurillo et al., 2005; Voelcker-Rehage and Alberts, 2005). The CFE test refers to a task that exerts a certain level of grip force, or precisely exerts maximal grip force in line with a target level in a sine or rectangular pattern. The CFE test has the advantage of not only obtaining the exercising ability, but also information on the neuromuscular control mechanism, because visual feedback can be captured in the differences between the target value and the participant's grip force exerted in the experiment. Thus, since the CFE test requires hand-eye coordination and grip force control, it can be effectively used to evaluate neuromuscular function (Nagasawa et al., 2000).
Damage in performance related to age, such as increase in injury from a fall, is due to decrease in the ability to control muscle power, rather than decrease in the ability for maximum performance (Schultz, 1992). The CFE test is considered to be more appropriate to objectively evaluate the current status of elderly people or patients, and to properly prevent injuries and rehabilitation.
Most existing studies have actually performed the CFE test based on the abduction force of the index finger. The first dorsal interosseous of the index finger is a major muscle controlling abduction, and an EMG signal can be obtained in a relatively easy and precise manner, without interference of the surrounding muscles. In addition, the first dorsal interosseous of the index finger has a simple mechanical action, and therefore it has been frequently used in many studies (Stephens and Taylor, 1972).
However, since most ADLs use all five fingers rather than just the index finger, there is a limitation in that an evaluation of the hand function cannot be fully made with only the index finger. This study conducted the CFE test using the multi-finger force measurement system (MFFM system) to complement such a limitation.
4.4 Relationship between age and hand function
The function of the neuromuscle that precisely controls hand force decreases as aging progresses (Galganski et al., 1993; Sosnoff and Newell, 2008), and this function is remarkably reduced after 50 years of age (Mathiowetz et al., 1985; Ranganathan et al., 2001; Bohannon et al., 2006) which causes a huge inconvenience to the ADLs of elderly people and disturbs independent living. The causes of deterioration in the motor control ability according to aging have been estimated to be the partial structural change in fingers, and nervous system change (Galganski et al., 1993; Carmeli et al., 2003). A CFE test can evaluate the change in function of the nervous system. The motor control ability is regarded as excellent when muscle contraction and relaxation is conducted softly with low fluctuation and high accuracy (Brown and Bennett, 2002). A smaller difference between target level and the subjects' exerted grip force in the CFE test indicates a better ability to control grip force. A study by Ranganathan et al. (2001) asserted that in a task constantly exerting pinch force, the ability for control in elderly people was inferior to that of young people. Nagasawa et al. (2000) and Voelcker-Rehange and Alberts (2005) also reported that the CFE test result in elderly people was significantly lower than that of young people. This implies that aging much affected the grip force controlling ability.
In order to examine the difference in grip force controlling ability according to age, this study performed a CFE test targeting elderly people and young people using the MFFM system. According to the result, 16% more tracking errors (rRMSE) were found in the elderly people group than in the young people group, which implies that the grip force controlling ability of the elderly people had decreased.
The grip force controlling ability represented by the tracking error showed a significant difference according to gender. Women's rRMSE was 10% larger than that of men's, which implies that the tracking task performing ability of women was lower than that of men. According to the result of a study by Nagasawa et al. (2000), aged women were inferior to aged men in terms of the CFE test. In addition, women were inferior to men in hand agility (Aniansson et al., 1979; Ruff and Parker, 1993) and response speed (Houx and Jolles, 1993). The difference in hand function according to gender is closely related to the movement experienced in everyday life, which can be inferred because there are more activities involving hands and upper limbs for men than for women (Wells, 1991).
Although the interaction effect between gender and age was not statistically significant (p = 0.06), the difference in tracking error between young and elderly groups in female were generally more obvious than those for the male group. In female, the tracking errors of elderly people were larger than those of young people. This means that the decline in hand function according to aging is more remarkable in women than in men. In this regard, continual monitoring of the hand function and training or rehabilitation treatment for elderly women is deemed to be required.
4.5 Relationship between tracking error and target force levels
The main effect of the target force level on the tracking errors was also statistically significant. Significantly large rRMSE values were obtained of 0.169 and 0.065 at the 5% and 15% MVCs, respectively, while significantly small rRMSE values (ranges from 0.042~0.048) were found in more than 25% MVC target force levels. These are similar to the results reported by Galganski et al. (1993) and Slifkin and Newell (2000), and it can be inferred that task exerting and maintaining of a small force require more accurate and difficult neuromuscular function control than that of a larger force. The difference in grip force controlling ability between elderly people and young people groups in this study was remarkable (except at target force levels of 35% and 55% MVCs). Since this means that elderly people have more difficulties in exerting a precise and small grip force exertion than young people, it is conjectured to be desirable not to place elderly people in industrial worksites where work on precise and minute grip force is required.
The interaction effect of target force level and gender was also statistically significant. At small target force levels (5% and 15% MVC), women showed larger tracking errors than men; while at the highest target force level (55% MVC), men showed larger tracking error values than women. This means that women feel greater difficulty in maintaining a small force than a large force, while men feel greater difficulty in maintaining a larger force than a small force. Women show a relatively stable trend in exerting a large force, while men show a relatively stable trend in exerting a small force. The larger tracking errors revealed in women upon controlling a minute force can be related to those in the study by Kamel (2003), where when comparing the same muscle group, the decrease in isometric muscle strength starts earlier in women than in men.
According to this study, the maximum grip strength was affected only by gender, not by aging; whereas, the CFE test (tracking error) was affected by both gender and aging. Thus, the CFE test might be more appropriate as a tool to evaluate hand function for elderly people.
4.6 Limitations of this study
The limitations of this study are that there was small a number of test subjects, and that diverse targeting tasks were not applied. In further study, greater diversity in subject groups is planned, and the adoption of various targeting tasks, such as sinusoidal and rectangular patterns, will be considered. A further relevant study has been planned to use the CFE test of this study for effective rehabilitation treatment.
The results of this study are conjectured to be applicable to physical treatment or rehabilitation. These results are also deemed to be useful as hand function evaluation guidelines, by complementing the limitations of current hand function evaluation tools used in clinical practice. In addition, the results of this study can be used as a tool for physiotherapy to improve hand function, and to prevent hand function decline in elderly people.
For maximum grip force, by age and gender, women exerted only 69.3% of the maximum grip force of men, and elderly people exerted only 91% of young people's maximum grip force.
The elderly people showed larger tracking errors than the young people, and larger tracking errors were observed for women than for men.
A larger tracking error indicates a lesser ability to control grip force. This indicates that the grip force controlling abilities of elderly people and women are inferior to those of young people and men. In addition, a larger difference was found in tracking errors according to women's age when compared to men's age. This means that the decline in hand function according to aging is more noticeable in women; and therefore it is considered that continuous monitoring of aged women's hand function is needed. The difference in grip force controlling ability between elderly people and young people at low target force level (5% MVC) was remarkable. This means that the controlling ability of elderly people for precise and small grip force is very low. In this regard, it is desirable to carefully consider placing elderly people in workplaces requiring precision work.
Because studies on hand functionality for Korean are lacking, this study could provides a basic method for evaluating hand function. These results can be used as guides for physiotherapy and rehabilitation designed to improve the hand function of patients or elderly subjects.
References
1. Aniansson, A., Rundgren, A. and Sperling, L., Evaluation of Functional Capacity in Activities of Daily Living in 70-year-old Men and Women. Scandinavian Journal of Rehabilitation Medicine, 12(4), 145-154, 1979.
Crossref
Google Scholar
2. Balogun, J.A., Akinloye, A.A. and Adenlola, S.A., Grip Strength as a Function of Age, Height, Body Weight and Quetelet Index. Physiotherapy Theory and Practice, 7(2), 111-119, 1991.
Crossref
Google Scholar
3. Bohannon, R.W., Peolsson, C.A. and Massy-Westropp, N., Consolidated Reference Values for Grip Strength of Adults 20 to 49 Years: A Descriptive Meta-Analysis. Isokinetics and Exercise Science, 14, 221-224, 2006.
Crossref
Google Scholar
4. Brown, S. and Bennett, E., The Role of Practice and Automaticity in Temporal and Nontemporal Dual-task Performance. Psychological Research, 66(1), 80-89, 2002.
Crossref
Google Scholar
PubMed
5. Carlton, L.G. and Newell, K.M., Force Variability and Characteristics of Force Production. In Variability and Motor Control, edited by K.M. Newell and M. Daniel, 15-36. IL: Human Kinetics books, 1993.
Crossref
6. Carmeli, E., Patish, H. and Coleman, R., The Aging Hand. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 58(2), M146-M152, 2003.
Crossref
Google Scholar
PubMed
7. Christou, E.A. and Carlton, L.G., Old Adults Exhibit Greater Motor Output Variability than Young Adults Only during Rapid Discrete Isometric Contractions. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 56(12), B524-B532, 2001.
Crossref
Google Scholar
8. Christou, E.A., Motor Output Variability. In Encylopedia of Movement Disorders, edited by Kompoliti, K., and L. Verhagen, 202-204. Oxford: Academic Press, 2010.
Crossref
Google Scholar
9. Christou, E.A., Aging and Variability of Voluntary Contractions. Exercise and Sport Sciences Reviews, 39(2), 77-84, 2011.
Crossref
Google Scholar
PubMed
10. Crosby, Carla A. and Marwan A. Wehbé, Hand strength: normative values. The Journal of hand surgery, 19(4), 665-670, 1994.
Crossref
Google Scholar
PubMed
11. Desrosiers, J., Bravo, G., Hébert, R. and Dutil, É., Normative Data for Grip Strength of Elderly Men and Women. American Journal of Occupational Therapy, 49(7), 637-644, 1995.
Crossref
Google Scholar
PubMed
12. Galganski, M.E., Fuglevand, A.J. and Enoka, R.M., Reduced Control of Motor Output in a Human Hand Muscle of Elderly Subjects during Submaximal Contractions. Journal of Neurophysiology, 69(6), 2108-2115, 1993.
Crossref
Google Scholar
13. Halaney, M.E. and Carey, J.R., Tracking Ability of Hemiparetic and Healthy Subjects. Physical Therapy, 69(5), 342-348, 1989.
Crossref
Google Scholar
PubMed
14. Hall, C., External Pressure at the Hand during Object Handling and Work With Tools. International Journal of Industrial Ergonomics, 20(3), 191-206, 1997.
Crossref
Google Scholar
15. Hanten, W.P., Chen, W.Y., Austin, A.A., Brooks, R.E., Carter, H.C., Law, C.A. and Vanderslice, A.L., Maximum Grip Strength in Normal Subjects from 20 to 64 Years of Age. Journal of Hand Therapy, 12(3), 193-200, 1999.
Crossref
Google Scholar
PubMed
16. Härkönen, R., Piirtomaa, M. and Alaranta, H., Grip Strength and Hand Position of the Dynamometer in 204 Finnish Adults. Journal of Hand Surgery (British and European Volume), 18(1), 129-132, 1993.
Crossref
Google Scholar
PubMed
17. Heyward, V.H., Johannes-Ellis, S.M. and Romer, J.F., Gender Differences in Strength. Research Quarterly for Exercise and Sport, 57(2), 154-159, 1986.
Crossref
Google Scholar
18. Houx, P.J. and Jolles, J., Age-related Decline of Psychomotor Speed-effects of Age, Brain Health, Sex, and Education. Perceptual and Motor Skills, 76(1), 195-211, 1993.
Crossref
Google Scholar
PubMed
19. Hortobágyi, T. and DeVita, P., Altered Movement Strategy Increases Lower Extremity Stiffness during Stepping Down in the Aged. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 54(2), B63-B70, 1999.
Crossref
Google Scholar
20. Jagacinski, R.J., Liao, M.J. and Fayyad, E.A., Generalized Slowing in Sinusoidal Tracking by Older Adults. Psychology and Aging, 10(1), 8-19, 1995.
Crossref
Google Scholar
PubMed
21. Jones, R.D., Measurement of Sensory-motor Control Performance Capacities: Tracking Tasks. In The Biomedical Engineering Handbook, edited by Bronzino J. D, 149.1-149.25. Boca Raton, FL: CRC Press, 2000.
Crossref
22. Kallman, D.A., Plato, C.C. and Tobin, J.D., The Role of Muscle Loss in the Age-related Decline of Grip Strength: Cross-sectional and Longitudinal Perspectives. Journal of Gerontology, 45(3), M82-M88, 1990.
Crossref
Google Scholar
23. Kamel, H.K., Sarcopenia and Aging. Nutrition Reviews, 61(5), 157-167, 2003.
Crossref
Google Scholar
PubMed
24. Kennedy, D.M. and Christou, E.A., Greater amount of Visual Information Exacerbates Force Control in Older Adults during Constant Isometric Contractions. Experimental Brain Research, 213(4), 351-361, 2011.
Crossref
Google Scholar
25. Kim, D.M. and Kong, Y.K., Development of an Adjustable Multi-Finger Force Measurement (MFFM) System for Research on Hand Tool-related Musculoskeletal Disorders. The Applied Human Factors and Ergonomics 2nd International Conference, Las Vegas, July, 14-17, 2008.
Crossref
26. Kong, Y.K. and Lowe, B.D., Optimal Cylindrical Handle Diameter for Grip Force Tasks. International Journal of Industrial Ergonomics, 35(6), 495-507, 2005.
Crossref
Google Scholar
27. Krampe, R.T., Aging, Expertise and Fine Motor Movement. Neuroscience & Biobehavioral Reviews, 26(7), 769-776, 2002.
Crossref
Google Scholar
PubMed
28. Kriz, G., Hermsdörfer, J., Marquardt, C. and Mai, N., Feedback-based Training of Grip Force Control in Patients with Brain Damage. Archives of Physical Medicine and Rehabilitation, 76(7), 653-659, 1995.
Crossref
Google Scholar
PubMed
29. Kubota, H., Demura, S. and Uchiyama, M., Effects of repeat training of the controlled force exertion test on dominant and nondominant hands. American Journal of Sports Science and Medicine, 1, 47-51, 2013.
Crossref
30. Kurillo, G., Bajd, T. and Tercelj, M., The Effect of Age on the Grip Force Control in Lateral Grip. Engineering in Medicine and Biology Society, 6, 4657-4660, 2004a.
Crossref
Google Scholar
PubMed
31. Kurillo, G., Zupan, A. and Bajd, T., Force Tracking System for the Assessment of Grip Force Control in Patients with Neuromuscular Diseases. Clinical Biomechanics, 19(10), 1014-1021, 2004b.
Crossref
Google Scholar
32. Kurillo, G., Gregoric, M., Goljar, N. and Bajd, T., Grip Force Tracking System for Assessment and Rehabilitation of Hand Function. Technology and Health Care, 13(3), 137-149, 2005.
Crossref
Google Scholar
PubMed
33. Lee, K.S., Woo, K.J., Shim, J.H. and Lee, G.H., The Clinical Study of Grip and Pinch Strength in Normal Korea Adults. Journal of the Korea Orthopaedic Association, 30(6), 1589-1597, 1995.
Crossref
34. Levine, L., Falkel, J.E. and Sawka, M.N., Upper to Lower Body Strength Ratio Comparisons Between Men and Women. Medicine & Science in Sports & Exercise, 16(2), 125, 1984.
Crossref
Google Scholar
35. Lexell, J., Henriksson‐Larsén, K., Winblad, B. and Sjöström, M., Distribution of Different Fiber Types in Human Skeletal Muscles: Effects of Aging Studied in Whole Muscle Cross Sections. Muscle & Nerve, 6(8), 588-595, 1983.
Crossref
Google Scholar
36. Martin, S., Neale, G. and Elia, M., Factors Affecting Maximal Momentary Grip Strength. Human Nutrition. Clinical Nutrition, 39(2), 137-147, 1985.
Crossref
Google Scholar
37. Mathiowetz, V., Kashman, N., Volland, G., Weber, K., Dowe, M. and Rogers, S., Grip and Pinch Strength: Normative Data for Adults. Archives of Physical Medicine Rehabilitation, 66(2), 69-74, 1985.
Crossref
Google Scholar
38. McMullin, D.L. and Hallbeck, M.S., Comparison of power grasp and three-jaw chuck pinch static strength and endurance between industrial workers and college students: A pilot study. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting, 36(10), 770-774, 1992.
Crossref
Google Scholar
39. McPhee, S.D., Functional Hand Evaluations: A Review. American Journal of Occupational Therapy, 41(3), 158-163, 1987.
Crossref
Google Scholar
PubMed
40. Miller, A.E.J., MacDougall, J.D., Tarnopolsky, M.A. and Sale, D.G., Gender Differences in Strength and Muscle Fiber Characteristics. European Journal of Applied Physiology and Occupational Physiology, 66(3), 254-262, 1993.
Crossref
Google Scholar
41. Nagasawa, Y., Demura, S., Yamaji, S., Kobayashi, H. and Matsuzawa, J., Ability to Coordinate Exertion of Force by the Dominant Hand: Comparisons among University Students and 65-to 78-year-old Men and Women. Perceptual and Motor Skills, 90(3), 995-1007, 2000.
Crossref
Google Scholar
42. Nagasawa, Y. and Demura, S., Development of an Apparatus to Estimate Coordinated Exertion of Force. Perceptual and Motor Skills, 94(3), 899-913, 2002.
Crossref
Google Scholar
PubMed
43. Nagasawa, Y. and Demura, S., Controlled Exertion of Force by Developmentally Delayed Young Men and Women. Perceptual and Motor Skills, 101(2), 487-497, 2005.
Crossref
Google Scholar
PubMed
44. Oldfield, R.C., 1971. The Assessment and Analysis of Handedness: the Edinburgh inventory. Neuropsychologia, 9(1), 97-113, 1971.
Crossref
Google Scholar
PubMed
45. Pheasant, S.T. and Scriven, J.G., Sex Differences in Strength: Some Implications for the Design of Hand tools. In Proceedings of the Ergonomics Society's Annual Conference, edited by Coombers. K, 9-13. London: Taylor and Francis, 1983.
Crossref
46. Ranganathan, V.K., Siemionow, V., Sahgal, V. and Yue, G.H., 2001. Effects of Aging on Hand Function. Journal of the American Geriatrics Society, 49(11), 1478-1484, 2001.
Crossref
Google Scholar
PubMed
47. Ruff, R.M. and Parker, S.B., Gender-and Age-specific Changes in Motor Speed and Eye-hand Coordination in Adults: Normative Values for the Finger Tapping and Grooved Pegboard Tests. Perceptual and Motor Skills, 76(3), 1219-1230, 1993.
Crossref
Google Scholar
48. Schmidt, R.A., Zelaznik, H., Hawkins, B., Frank, J.S. and Quinn, Jr. J.T., Motor-output Variability: A Theory for the Accuracy of Rapid Motor Acts. Psychological Review, 86(5), 415-451, 1979.
Crossref
Google Scholar
PubMed
49. Schultz, A.B., Mobility Impairment in the Elderly: Challenges for Biomechanics Research. Journal of Biomechanics, 25(5), 519-528, 1992.
Crossref
Google Scholar
PubMed
50. Shim, J.K., Lay, B.S., Zatsiorsky, V.M. and Latash, M.L., Age-related Changes in Finger Coordination in Static Prehension Tasks. Journal of Applied Physiology, 97(1), 213-224, 2004.
Crossref
Google Scholar
51. Slifkin, A.B. and Newell, K.M., Variability and Noise in Continuous Force Production. Journal of Motor Behavior, 32(2), 141-150, 2000.
Crossref
Google Scholar
PubMed
52. Smith, C.D., Umberger, G.H., Manning, E.L., Slevin, J.T., Wekstein, D.R., Schmitt, F.A. and Markesbery, W.R., Critical Decline in Fine Motor Hand Movements in Human Aging. Neurology, 53(7), 1458-1458, 1999.
Crossref
Google Scholar
PubMed
53. Sosnoff, J.J. and Newell, K.M., Are Age-related Increases in Force Variability Due to Decrements in Strength? Experimental Brain Research, 174(1), 86-94, 2006.
Crossref
Google Scholar
54. Sosnoff, J.J. and Newell, K.M., Age-related Loss of Adaptability to Fast Time Scales in Motor Variability. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 63(6), P344-P352, 2008.
Crossref
Google Scholar
55. Stephens, J.A. and Taylor, A., Fatigue of Maintained Voluntary Muscle Contraction in man. The Journal of Physiology, 220(1), 1-18, 1972.
Crossref
Google Scholar
PubMed
56. Talsania, J.S. and Kozin, S.H., Normal Digital Contribution to Grip Strength Assessed by a Computerized Digital Dynamometer. Journal of Hand Surgery (British and European Volume), 23(2), 162-166, 1998.
Crossref
Google Scholar
57. Trossman, B. and Li., P.W., The Effect of the Duration of Intertribal Rest Periods on Isometric Grip Strength Performance in Young Adults. Journal of Hand Surgery [British Volume], 23(2), 162-166, 1989.
Crossref
Google Scholar
58. Vaillancourt, D.E. and Newell, K.M., Aging and the Time and Frequency Structure of Force Output Variability. Journal of Applied Physiology, 94(3), 903-912, 2003.
Crossref
Google Scholar
PubMed
59. Van Beers, R.J., Haggard, P. and Wolpert, D.M., 2004. The Role of Execution Noise in Movement Variability. Journal of Neurophysiology, 91(2), 1050-1063, 2004.
Crossref
Google Scholar
PubMed
60. Voelcker-Rehage, C. and Alberts, J.L., Age-related Changes in Grasping Force Modulation. Experimental Brain Research, 166(1), 61-70, 2005.
Crossref
Google Scholar
61. Wells, C.L., Women, Sport & Performance. IL: Human Kinetics Books, 1991.
Crossref
PIDS App ServiceClick here!